
Cows Milk AllergyFactsheets
Does My Child Have a Cow’s Milk Allergy?
This factsheet has been written to help you understand and gain some advice on suspected cow’s milk allergy in babies...
 Helpline01322 619898
Helpline01322 619898For each of the eight Milestones we explain what to expect with advice from experts in allergy.
Allergy UK, the leading charity for people living with all kinds of allergic conditions, has launched a new resource pack for parents whose child has been diagnosed with cow’s milk allergy. The pack, designed as a Roadmap, tackles the challenges of feeding and caring for children with cow’s milk allergy, step by step. It focuses on eight key milestones from diagnosis and management through to the stage when a child might outgrow the condition, providing practical advice and information along the way.
Supported by Reckitt Benckiser, each milestone Factsheet includes comments from a parent of a child with the condition, highlighting their own experiences, anxiety and concerns around caring for a child with cow’s milk allergy. Around 2% of babies have a diagnosed cow’s milk allergy and research has shown that parents are anxious about the condition and want more information about the future wellbeing of their infant. This Roadmap will provide you with the support and information you need in milestones that align with your baby’s development.


How do I manage my baby’s cow’s milk allergy?
If you and your baby have seen your healthcare professional and have been given a diagnosis of cow’s milk protein allergy, you may be wondering what to do next. These milestones provide you with information to help you proactively manage your baby’s cow’s milk allergy and the possible reintroduction of cow’s milk into their diet.
What is a cow’s milk allergy?
In case you are still wondering what the diagnosis means, here is a short explanation: Cow’s milk allergy (also referred to as CMA) is a reaction to the proteins found in cow’s milk. Generally, symptoms of an allergic reaction to cow’s milk will appear either immediately (within minutes up to one or two hours ) after eating or drinking food containing cow’s milk protein (suggesting an IgE mediated reaction) or the reaction may be delayed – occurring up to 48 hours later (suggesting a non-IgE mediated reaction).2 For some babies the reactions may be mixed, appearing immediately and at times, delayed.1 You will find links to more information at the end of this section.
Nathalie is a mum who knows only too well the journey you go on after your baby is diagnosed with cow’s milk allergy…
When my son was diagnosed I certainly wondered what to do next! I believe that this information will help in providing the support and information you need at this anxious time – Nathalie Newman, Allergy mum and advocate.
What is the difference between immediate and delayed milk allergy?
Immediate Onset: Symptoms appear within one or two hours.
Delayed Onset: Symptoms appear up to 48 hours later.
What does this diagnosis mean for my baby?
The majority of children outgrow milk allergy. Overall, a high percentage of children fully outgrow a milk allergy or gain some tolerance (for example, small amounts of milk protein baked within a biscuit) by the age of five and usually much sooner. Children that persist with a milk allergy past the age of five years old are less common but they may still go on to outgrow this in their teenage years.
Your GP or allergy specialist will work with you, usually with the help of a dietitian,5 to actively manage your child’s CMA which will give them the best chance to outgrow their allergy. Read more about this in Milestone 2. Whilst many babies may have immediate relief after removing cow’s milk from their diet, for other babies, it can take longer than the two-to-four-week recommended time frame for symptoms to resolve, especially if they have more severe symptoms. It’s important to get support during this time. After symptoms have cleared, your healthcare professional may discuss carefully introducing cow’s milk protein back into your baby’s diet, either through your breast milk, formula choice or baked milk.
It’s not unusual to feel anxious or stressed after receiving the diagnosis. Please seek help if you feel overwhelmed by this stress.
How can I cope with anxiety about my child’s allergy?
Managing your child’s allergies can be worrying, but remember that you are not alone. It is very common to feel anxious after this diagnosis but it is possible for you and your baby to lead a normal happy life alongside a food allergy. Your healthcare support team, family, other parents and friends are important supporters in your journey. Planning ahead, especially before going out, can also help to alleviate your concerns. Allergy UK have many resources to help you.
What should I do if my baby still has symptoms?
If you are concerned after diagnosis that your baby is still experiencing symptoms, even though you have removed milk from their diet, you should talk to your healthcare professional about your baby’s ongoing care. Your healthcare professional may refer you and your baby to a dietitian if your baby’s symptoms are mild to moderate. However, if symptoms are severe you may be referred to a children’s specialist allergy service.
It‘s also helpful to record your baby’s symptoms in a food allergy and symptoms diary. Your healthcare support team will use this information to understand the relationship between your baby’s symptoms and the food they’ve had. Recording symptoms will also help your healthcare professional decide if any tests are required and help them to distinguish allergic reactions from other causes and confirm whether it is delayed or immediate onset cow’s milk allergy.
Cow’s milk allergy is one of the most common food allergies in babies and young children.
Why change my baby’s feeding?
You will have been advised to avoid feeding your baby anything that contains cow’s milk protein. However, you are probably aware that many of the foods we consume daily contain cow’s milk, which provides an important source of energy, protein, vitamins and minerals both for you and your growing baby. But the fact is that it also contains the protein that causes allergy in some people. So, it’s important to understand that avoiding cow’s milk is not a long-term solution. The aim is to reintroduce milk protein when possible and this Roadmap is designed to help guide you through that process.
The goal of managing cow’s milk allergy is to exclude cow’s milk and foods containing cows’ milk totally for an agreed time frame, with the aim of reintroducing it later. Often milk products can begin to be introduced from 12 months of age, although this does vary.
When your child is at the stage where their tolerance to cow’s milk protein can be assessed, then cow’s milk may be carefully reintroduced, step by step, into your baby’s diet under the supervision of your healthcare professional. The way in which this is done is different depending on whether your child has an immediate or delayed reaction to milk, you will find more about this in Milestones 6 and 7.
Should I continue breastfeeding?
While it is rare, some babies can have an allergic reaction to cow’s milk protein consumed by Mum and passed to her baby through her breastmilk. If you have been able to successfully breastfeed then we encourage you to continue because of the many benefits for both you and your baby. Breastfeeding provides all the nourishment that a young baby needs, as well as many other benefits, such as antibodies. The nutrients in breast milk are easily digested and absorbed and your milk continually changes to meet your baby’s needs. If you are breastfeeding and your baby has allergic symptoms (for example diarrhoea and/or eczema), discuss a cow’s milk-free diet with a dietitian because it is important that breastfeeding mums have a healthy balanced diet.
It is recommended that you take Vitamin D (10 mcg) and calcium (1000 mg) supplements until you are able to speak to a dietitian. Vitamin D aids the absorption of calcium and helps to
keep teeth and bones healthy. In the UK all breastfed babies from birth to one year of age should be given a daily supplement of 8.5-10mcg of vitamin D.
It is really important for you to know that you can feed your child successfully whether you are breast or bottle feeding. This Milestone is intended to take some of the worry out of feeding your child. Working with a dietitian can also help to provide support and confidence especially when it comes to weaning – Nathalie Newman, Allergy mum and advocate.
What if I’m breast and/or formula feeding?
If you are not breastfeeding or are mixed feeding, your healthcare professional will advise you on the most suitable ‘hypoallergenic’ formula milk for an infant with a cow’s milk allergy.
If your baby did not show any allergic symptoms on breast milk alone and the symptoms appeared only when cow’s milk-based ‘top-up’ feeds were given, you should continue breastfeeding and continue to consume cow’s milk in your diet. You may wish to return to breastfeeding only. However, if this is not possible, and ‘top-up’ feeds are needed, your healthcare professional may advise you to replace cow’s milk-based formula with hypoallergenic infant formula.
It is worth noting any baby who has less than 500ml formula per day should also be given a vitamin D supplement of 8.5- 10mcg per day.
What is a “hypoallergenic formula”?
The word “hypoallergenic” means low allergy. The two recommended formulas for babies under six months with cow’s milk allergy are:
Soya is unsuitable under six months of age due to natural phyto oestrogens, but fresh soya milk can be tried in cooking from six months of age (for example, in family meals such as white sauce for lasagne) and as the main drink from the age of one year. Soya infant formula is available to buy from the age of six months old. Some infants may also react to soya, so exclude if you see symptoms similar to cow’s milk allergy returning (this is less likely in the immediate type allergy). Milk alternatives such as almond, oat or coconut milk have poor nutritional value compared with cow’s milk and are not suitable for infants. However, they may be used when cooking meals for the family. Rice milk should not be used for children under four and a half years of age.
What is an extensively hydrolysed formula (eHF)?
eHFs contain proteins that have been broken down into smaller segments so they are less likely to cause an allergic reaction and are therefore suitable for 90% of babies with cow’s milk allergy. They are either whey or casein-based, which are different types of milk proteins, and it’s important to discuss the best option with your healthcare professional. Some eHF’s contain pre- and probiotics that promote the growth of good bacteria in the gut and some eHFs with specific probiotics may also help to speed up the process of returning to cow’s milk.
For adults it may seem that eHFs have an unpleasant taste, but remember that babies experience taste differently from an adult and therefore they are more likely to accept an eHF. There are allergy formulas available that are halal and kosher certified, please ask your healthcare provider.
What is an amino acid formula (AAF)?
AAFs are based on the individual building blocks (amino acids) that make up a protein. Amino acid formulas are recommended on the rare occasion that a baby continues to have symptoms of cow’s milk allergy on an extensively hydrolysed formula (eHF) after two to four weeks, or when it is not an appropriate first choice for a baby with severe allergic reactions. It should be noted there are halal and kosher certified allergy formulas available, please speak to your prescriber.
Your healthcare professional will advise you on the most suitable ‘hypoallergenic’ formula milk.
What if my baby is older?
Hypoallergenic formulas are available for different age groups of babies with cow’s milk allergy, from birth up to young children, it is recommended to be prescribed up to the age of two years old. You can also use alternative milks such as soya, almond, hemp, oat or coconut once your child is two years old, or sooner if advised by your healthcare professional and rice milk once your child is over fourand- a-half years old. Many alternative milks have adequate calcium as long as you do not buy organic versions, but they are often lower in energy and protein than cow’s milk. Make sure you keep track of your child’s growth in their
red book.
Are there special preparation instructions for hypoallergenic formulas?
For further information on how to prepare infant formula, refer to the manufacturer’s website, your healthcare professional, dietitian or NHS Choices.
This factsheet has been written to help you understand and gain some advice on suspected cow’s milk allergy in babies...
Cow’s milk allergy occurs when the body’s immune (defence) system mistakenly recognises the proteins found in cow’s milk as harmful...
How has my child’s poo been affected by a milk allergy?
After your child has been diagnosed with a cow’s milk allergy you may be confused about what is ‘normal’ for their poo. Among the many recognised symptoms of cow’s milk allergy are abnormally loose, frequent poos, excessive straining, abdominal discomfort, painful wind and blood +/- mucus in the poo.6 You may be very worried that these symptoms are not settling when other symptoms have improved, but commonly, symptoms can take time to resolve.
What are normal stools for a baby diagnosed with a milk allergy?
Firstly, once your baby has moved to a milk-free diet it may take many weeks for their poo to settle down from the previous irritation from milk protein. Mucus which often looks like a stringy white/clear substance in your baby’s nappy may also take many weeks to calm down. Remember that it can be normal for mucus to appear in small amounts at other times, for example when your child has a cold or is teething.
The gut may take many weeks to settle down after a diagnosis of milk allergy and it is completely safe and normal for your child to have green poo whilst on an allergy formula.
If you feel worried that your baby still has more frequent poos than you’d expect, then think about some other factors. Consider whether your baby is gaining weight, as expected for them; are they having at least five wet nappies a day; are they alert and do they appear generally well. If you still feel concerned then you should contact your healthcare provider to discuss your worries. As your child gets older, there is a broad range of what is ‘normal’.
We know the frequency of poo reduces over the first year of life (on average from five to six times per day down to two) in babies who have not had a milk allergy, so you may find your child differs from this. There are times when a baby might strain or cry when passing a poo, which is often normal and settles with time. We also know that breastfed babies may be different from formula-fed babies. A breastfed baby may do a poo after every feed, or not for a few days, and this is in line with what is expected.
What about the colour of my baby’s poo?
Whilst we are usually looking for mustard or brown coloured poo this may change at times in babies who have a milk allergy. It might come as a surprise that a green poo for babies on an allergy formula is completely normal and not something to worry about. However, if your baby has black/coffee ground coloured poo or poos that look like redcurrant jelly or white poo then this is the time to seek medical advice.
What about constipation?
Constipation can often occur in combination with other symptoms for babies with a milk allergy. If your child is on medication or thickeners in milk for symptoms of reflux or sickness then these may also cause constipation. At times, a change to a milk-free diet can cause this symptom for the first time and it can take time to develop a regular toilet pattern.
Constipation is considered to be fewer than three poos per week (excluding breastfed babies), hard large poos or ‘rabbit droppings’, distress, straining or bleeding with hard poo. Try some first-line measures such as gently ‘cycling’ your baby’s legs (lie your baby down and gently move their legs as though they are riding a bicycle), encouraging plenty of fluids (if weaning, encouraging water from a sippy cup) and, if eating food, encouraging plenty of fruit and vegetables. If the constipation is causing real concern then discuss this with a GP/health visitor. Keeping a diary of the types of poo your baby is passing can help work out if there is a concern.
I do think that understanding a bit more about the Microbiome really helps as you navigate this journey. Knowing why it is important to have a wide range of foods in your baby’s diet is really helpful – Nathalie Newman, Allergy mum and advocate.
What about longer-term gut health?
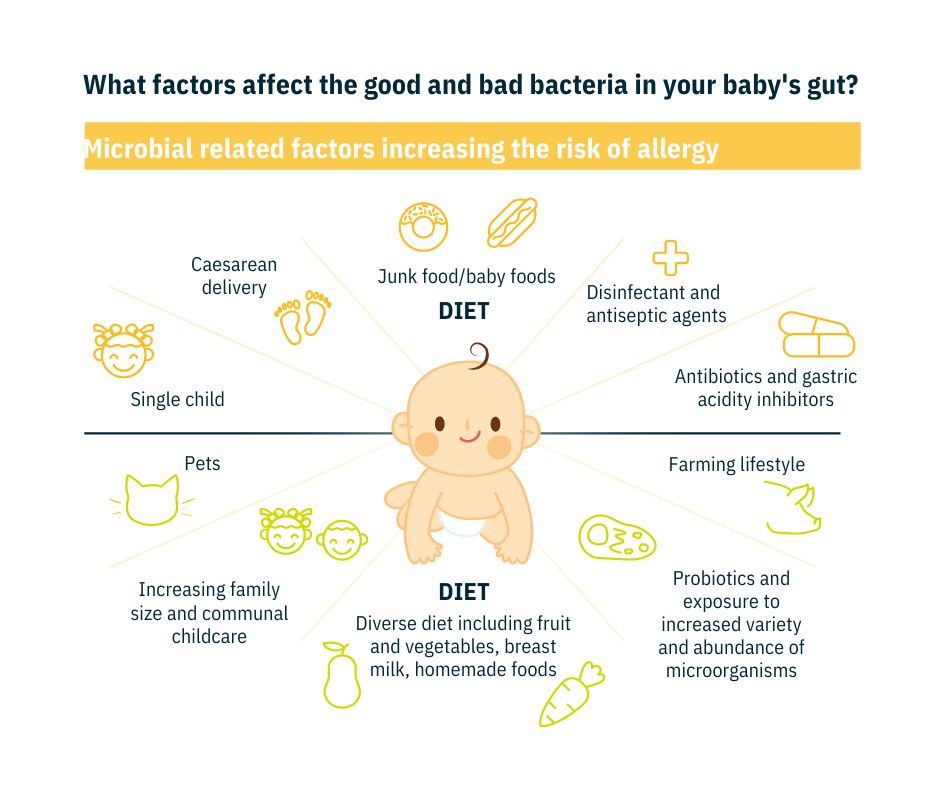
It is well known that the gut has a complex balance of trillions of tiny microorganisms or microbes (viruses, bacteria and fungi) that live inside our bodies. These microbes and how they function in the gut are referred to as the gut microbiome. The microbiome helps to produce vitamins, support our immune system and assist in the development of our gut. For our long term health, and possibly to help support outgrowing a milk allergy, research has suggested the microbiome plays a part. Not all the mechanisms are understood and this is just one factor in a complex picture.
Our microbiomes need many different types of microbes to function well. There are many reasons for our microbiome to become unbalanced (many reasons that we cannot change) as highlighted in the picture. This imbalance of microbes on and in our bodies, can affect our immune system and may trigger responses contributing to diseases or allergies.
Scientists are currently trying to understand more about how our microbes work together in the microbiome during childhood and how its disruption might
lead to illness. It is important to ensure that the balance of our gut microbes is restored early in life, when we’re babies, to give us the best chance of avoiding food allergies.
How does diet affect the microbiome?
In weaning, feeding your baby a wide range of foods helps their gut microbiome develop. The age when a baby starts eating allergenic food also influences whether they may develop food allergies. When they are ready, offering your baby different kinds of fruits, vegetables and a wide variety of foods (See Milestone 5) reduces
their chances of developing food allergies.
Some studies have shown that giving babies specific types of probiotics (these are live bacteria that have health benefits) and prebiotics (these are the food that helps the growth or activity of helpful microbes) may make them less likely to develop allergies. Not all types of probiotics have the same effect, for example, probiotics can be beneficial in different ways and the way one strain works is not the same as another. Some studies have shown that some types of probiotics may help children with cow’s milk allergy outgrow their allergy sooner. This benefit may not be the same for all probiotics.
Why is earlier exposure to allergens helpful?
Diet also has an impact on our gut microbes and allergy tolerance. Ensuring that children eat a variety of fruits, vegetables and a wide range of foods from an early age, will help in reducing food allergies. Read more about healthy diet and weaning, in Milestone 5.
When will my child outgrow their cow’s milk allergy?
It can be difficult to give a definite answer to this question when your child has been diagnosed with a cow’s milk allergy. But we do know from research that this is one of the allergens that are most likely to be outgrown. Most children will become tolerant of cow’s milk anywhere from one to five years of age1 whilst for other children tolerance might develop in their early teenage years. Babies who develop delayed symptoms are more likely to become tolerant sooner, compared with children who have experienced immediate reactions.
Will my child have other allergies in the future?
Research tells us that babies with cow’s milk allergy are two to four times more likely to experience other conditions such as eczema (over two times), gut symptoms, wheezing (four times), respiratory allergies (over three times) and other food allergies than those without food allergies. Whilst older children may suffer from asthma and nasal allergies like hayfever.
Food allergies are not the only predictors of whether a child may suffer from allergies in the future. The development of future allergies may depend on whether the baby’s
parents have also suffered from allergies in their lives (hereditary) and the environment around the baby, such as exposure to pets, dust, pollen and other environmental allergens. The gut microbiome may also play its part.
Wondering whether your child will have allergies in the future is a natural concern for us parents and you will want to know how likely this is. While there are a number of factors in this, knowing what to look out for is probably the most important – Nathalie Newman, Allergy mum and advocate.
How should I prepare and plan for my baby or child?
The more immediate future and how to plan for every day to make life as normal as possible may be a worry for you and your family. The good news is that this is achievable, with forward planning and educating and informing others who have responsibility for caring for your child.
If your child goes to nursery or school, or you have other childcare provision, then those caring for them in these environments need a good understanding of your child’s allergies through adequate training. An appropriate management plan for your child is important because this will give you some reassurance when your child is not in your care. A common example of a management plan for immediate food allergy would be from BSACI: Paediatric Allergy Action Plans.
There may be other events that need more planning like children’s parties, family gatherings, eating out and travelling abroad. Try taking foods with you, always ask about allergies and don’t be afraid to speak up. Take with you any allergy relief medication that your baby has been prescribed if they have an immediate allergy. For more information about managing, shopping, travelling, and starting in childcare settings please see Allergy UK’s Factsheets below.
As a parent with a child with food allergies we recognise it is not easy in these situations and you require support, as well as your child.
How can I help my child outgrow their milk allergy quicker?
Proactive management with support from a healthcare professional means slowly reintroducing small amounts of cow’s milk protein in the baked form e.g. a biscuit to help your child get back to cow’s milk. The age of your child, location and how this is done is unique to each child but is often around the one year of age mark.
Healthcare providers have shifted their focus to not keeping children on overly restricted diets for long periods as this does not help tolerance in infants. Read more about this in Milestones 6 and 7.
If your child is well but continues to have allergy symptoms, consider keeping a food and symptoms diary. In Milestone 1 of this roadmap, we mentioned this helpful document to record symptoms and food eaten. However, you can also add things like seasons, contact with animals, bowel habit, any skin flare-ups or other information about things around your baby or child that may also be causing allergy symptoms.
Early Years care is defined as all childcare settings, including childminders, preschools and nurseries, for children from birth to five...
This Factsheet explores the vicious cycle of anxiety, how to manage the physical sensations of anxiety and the link between...
When should I start weaning my baby who has a cow’s milk allergy?
For many years in the UK the recommended time to start weaning or introducing foods has been from around six months old when your baby is developmentally ready.1 While this remains the UK recommendation for all babies, research has suggested that starting earlier than this may be of benefit for some babies at risk of allergy.
If your baby is considered at high risk of allergies (babies with eczema or who already have a food allergy), earlier weaning may be considered, but not before 17 weeks. You will need to consider if your baby is developmentally ready (if your baby was born prematurely then seek advice about when the time is right for your baby).
Signs of readiness include being able to sit with support in a high chair with their head steady, trying to reach out to grab food and put it in their mouth, loss of the “tongue thrust reflex” (babies who aren’t ready, push the food back out with their tongue, so they get more round their face than they do in their mouths).
If you do wean your baby earlier than at six months, it is advised that you start with puréed foods.2 The baby-led weaning approach is safe for babies aged six months or older. Read more about this later in this Milestone.
Babies at risk of allergy may benefit from earlier introduction of weaning foods but not before 17 weeks.
What should I know about weaning my baby who has CMA?
Start by offering your baby small amounts of food, such as soft vegetables, fruit, starchy foods (like potato, sweet potato, milk free baby rice), protein foods (like chicken, meat, fish) or vegetable protein (like lentils or chickpeas), in textures appropriate for your baby’s age. Adding salt and sugar is not needed. Some parents may prefer baby-led weaning, which means offering your baby only finger foods and letting them feed themselves from the start, rather than spoon-feeding them puréed or mashed foods. Of course, you can also choose to try a combination of both approaches. Babyled weaning should only be done from six months when it’s safer for babies.
A wide range of tastes and textures from all the food groups (this may include homecooked or commercial products) should be given, but not those that contain cow’s milk as an ingredient. You need to carefully check the ingredients list on food items for milk protein and avoid foods that contain any of the following
Make sure you read food labels carefully. Foods packaged within the European Union are required by law to include allergen information. Ingredient lists on food labels have to clearly highlight that they contain specific allergens. Read more about food labelling here. Here’s an example of a label showing a milk allergen in bold:
INGREDIENTS:
Water, Vegetable Oils (37%) (Rapeseed Oil, Palm Oil), Olive Oil (22%), Whey Powder (from Milk), Salt (1.1%), Emulsifier (Mono- and Diglycerides of Fatty Acids), Stabiliser (Sodium Alginate), Preservative (Potassium Sorbate), Colour (Carotones), Flavouring, Vitamin A, Vitamin D.
For more information about a milk-free diet and how to ensure you are meeting nutritional goals for your child with a cow’s milk allergy, please read our leaflet: Cow’s Milk-Free Diet information for Babies and Children.
Will diet help with managing my baby’s CMA?
Giving your baby a variety of foods, alongside breast or formula milk, will help set your child up for a lifetime of healthier eating. If your baby’s diet has an abundance of fruits, vegetables and a wide range of foods, this may lower the likelihood of food allergy by the time your baby is two years of age. Gradually, you’ll be able to increase the amount and variety of food your baby eats until they can eat the same foods as the rest of the family, in smaller portions. In the beginning, how much your baby eats is less important than getting them used to the idea of eating, as they’ll still be getting most of their energy and nutrients from breast milk or infant formula.
Can I feed my baby foods that are known to cause allergies?
Feeding your baby other well-known allergens like egg and peanut has been shown to help lower the chances that your baby will be allergic to these foods.2 For this reason it is encouraged to introduce foods like cooked egg, and then smooth peanut butter early in the weaning process, followed by other foods known to cause food allergies.
It is encouraged when weaning to have a diverse diet from an early age. Try any new higher allergen food from the following list individually, when your baby is well, early in the day and ensure you start with small amounts of each food and gradually build up. It is recommended that foods that are known to cause allergies are also introduced as part of a varied diet from weaning.
Only give your baby foods in a form that is age-appropriate, to avoid the risk of choking.
It is very important that once introduced. and there is no reaction, you should keep offering those foods as part of your baby’s usual diet, to minimise the risk of allergy. By frequently giving these foods it helps continue to reduce the risk of your child becoming allergic to them. For more support with introducing these foods please see the BSACI Infant feeding
and allergy guidance or Allergy UK Weaning Support Pack.
I remember that weaning was a particularly worrying time. Keeping a food diary was so helpful because it meant that I could keep track of the food offered and, importantly, keep a note of any reactions – Nathalie Newman, Allergy mum and advocate.
How do I monitor if my baby is reacting?
Pay attention to any reactions your baby may experience when feeding. Immediatetype allergic reactions (which are rare) usually happen within a minute or two or up to two hours after eating the food. Reactions may vary in their severity. Keep note of any foods you are concerned about, including any possible reactions. If your baby shows no reaction immediately after feeding, remember to also keep an eye out for any delayed reactions that your baby may show hours after eating. If you are concerned about a potential reaction, make sure you consult a healthcare professional. You should seek attention as soon as possible if an immediate reaction has occurred. For more information on symptoms can be found within our Cow’s
Milk Allergy Factsheet.
Don’t continue to feed your baby something they are reacting to. If you think your baby may be having an allergic reaction, seek medical advice.2 If you are worried about introducing new foods or foods that have previously caused an immediate reaction in your baby, then consider discussing a prescription for antihistamines with your healthcare professional.
This Factsheet has been written to provide information on introducing solid foods to babies and includes information about introducing foods...
We know that being a parent isn’t easy at the best of times, so when you add a poorly baby...
We know that being a parent isn’t easy at the best of times, so when you add a poorly baby...
What are the benefits of re-introducing cow’s milk protein?
Finding ways to provide your child with cow’s milk in their diet is not only important for their diet but it will also reduce the anxiety and inconvenience of having to maintain a milk free diet. Cow’s milk provides us with energy, protein, calcium, vitamins and other minerals. Although we get some of these nutrients from other foods, milk products provide us with much of the calcium we need. Cow’s milk is found in many of the everyday foods we have available, which is why it’s probably the most difficult allergen to avoid. It’s used in the manufacture of many nutritionally important foods, such as yogurt and cheese.
The aim is to re-introduce cow’s milk gradually, step by step, back into your baby’s diet. The process of building up to having fresh cow’s milk is followed according to the milk ladder ideally with the support of a healthcare professional, which you can read more about in Milestone 7.
When will my child be ready for milk introduction?
The time it takes for a baby to be ready to have cow’s milk in their diet again, is different for each baby. Many children outgrow their allergy during childhood1 and can have milk in baked form before dairy products or fresh milk. Most children will grow out of their cow’s milk allergy by five years of age or before with, persistent milk allergy less common. The process of milk reintroduction will differ depending on whether your baby has had an immediate or delayed reaction to milk for safety reasons.
How is milk reintroduced in delayed (non IgE) milk allergy?
If your baby has delayed onset allergy and been on a milk free diet for around six months they may be able to have baked milk introduced between the age of nine to twelve months to see if they have outgrown their allergy. Your healthcare professional will assess whether your child has started to outgrow their milk allergy. Based on their judgement, they may then advise you to introduce cow’s milk back into their diet, as milk is an important part of their diet for the long-term. Tolerance is often achieved more quickly with delayed reactions to milk, but support is needed to ensure an adequate diet and growth and to fully understand how to progress.
This can be a bit daunting and the guidance of your consultant or dietitian is vital. If your child is ready they will provide you with a milk ladder to follow, along with the advice you will need on how to slowly introduce foods containing cow’s milk and what to watch out for – Nathalie Newman, Allergy mum and advocate.
How is milk introduced for an immediate (IgE mediated) milk allergy?
If your baby has immediate onset IgE milk allergy you may be advised to reintroduce baked milk into the diet from the age of twelve months if your baby is ready. This must only be started on the advice of your healthcare professional after they have carried out an assessment, most likely including either skin prick tests or blood tests. In the past, doctors would advise parents not to feed their child any dairy. However, more recent studies have shown that slowly re-introducing milk in a baked form, for example, a small amount of biscuit, may help to achieve tolerance quicker. But each child needs to be assessed individually due to safety. Whilst it is important to help your child gain tolerance remember that not all children will start at the same time.
A slower milk reintroduction might be recommended. For some children this may take place when you are with a healthcare professional at an allergy centre or hospital so that your baby is in safe hands in case of a severe allergic reaction. Other children may be able to have baked milk introduced at home, but they will be assessed on an individual basis. It is important to remember that tolerance to baked milk does not mean a child has outgrown their milk allergy yet, but it is the first step in working towards this. It is then important your child is assessed regularly on how to progress, alongside monitoring growth and nutritional adequacy of the diet.
Where can I get support and what if my baby has an allergic reaction?
Always listen to the advice of your healthcare professional or dietitian. Reintroduction of cow’s milk at home should only be done if you have been advised to do so and received clear guidance on how to start. If the symptoms return, stop the reintroduction and inform your healthcare professional or dietitian. If your baby is unwell with an immediate reaction or significant delayed reaction then please seek medical help straight away.
A food and symptoms diary may be helpful when reintroducing foods back into the diet.
If you are frequently experiencing unexplained symptoms after meals it might be more than just a passing discomfort. Unidentified food...
What is the milk ladder and why am I being asked to follow it?
Milestone 6 of this roadmap, explains the importance of reintroducing cow’s milk back into your baby’s diet if appropriate to do so. If your baby has delayed onset cow’s milk allergy, without any signs of eczema, and has not had any immediate allergic reactions, then your healthcare professional may advise you to reintroduce cow’s milk protein in small amounts, once you have followed several months of exclusion. Generally, babies with delayed (Non-IgE) cow’s milk allergy are advised to follow a cow’s milk free diet until nine to twelve months of age, or for around foursix months. It is recommended that this should be done with the support of a healthcare professional or dietitian.
For the milk ladder in immediate cow’s milk allergy (IgE mediated) please see Milestone 6. If your child has had an immediate reaction to milk, reintroduction of tiny amounts of baked milk is also important to gain early tolerance but should be guided by a healthcare professional, especially if symptoms have been more severe or in older children. If your child has been diagnosed with a condition called FPIES, milk ladders should not be used and reintroduction in hospital (around age two) is normally recommended.
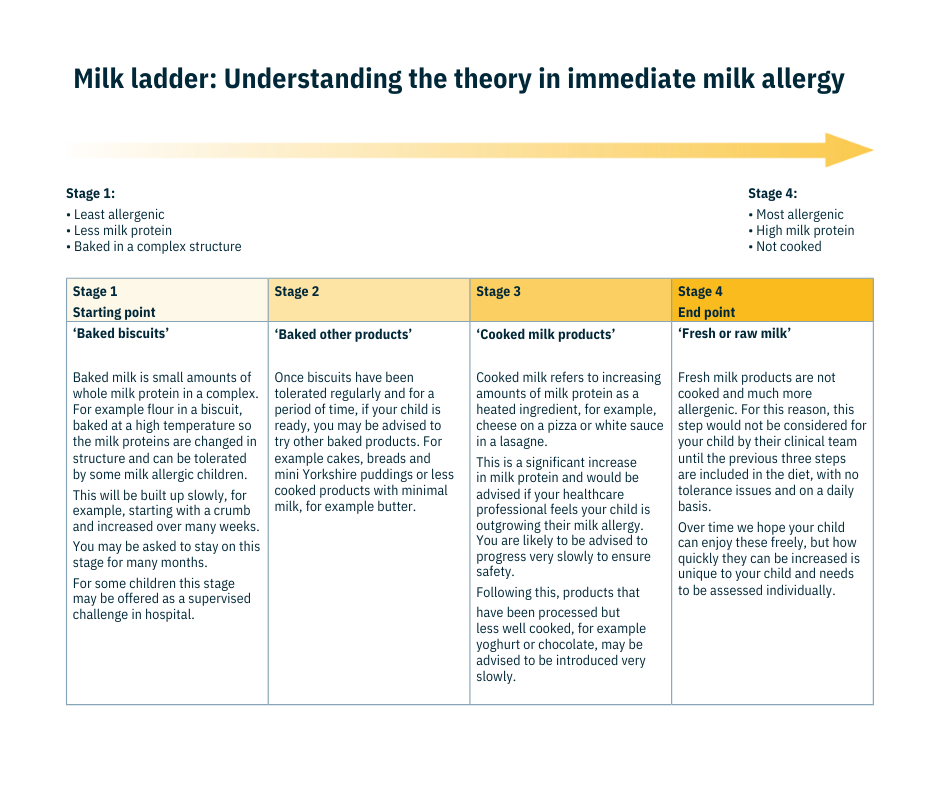
What is the milk ladder?
Reintroduction of cow’s milk is done gradually, according to something called the ‘milk ladder’. To begin with, milk in a form that is least likely to cause an allergic reaction is given. Then, as the baby shows minimal delayed symptoms or no reaction, less broken-down forms of milk are given until they can have fresh milk without a reaction. The milk ladder starts with wellcooked (baked) milk products because this is the form of milk least likely to cause an allergic reaction. The presence of flour is also important in binding with the baked milk and making it less allergenic. When milk is heated or ‘baked’, the protein is changed into a less allergenic form and so your baby/infant can tolerate this form first. If your baby shows no allergic reaction, then lightly cooked milk products (less baked) or heated milk products without flour are given until finally uncooked fresh milk can be tried when recommended.
Will following the milk ladder help my baby and me?
Following the milk ladder, starting with baked milk, will help your baby get back to milk faster than avoiding cow’s milk completely. As they become tolerant and have very mild or no reactions, you can then give more forms of cow’s milk according to the milk ladder. Don’t be disappointed if this takes time. All children are different and some may become tolerant after their first year, some by age two to three, school age or sometimes a bit longer. Some children continue to have poor tolerance to fresh milk, but this is not a big problem as alternatives are readily available.
Understanding the milk ladder and why you have been asked to follow is a good start for this Milestone. From my experience I would say take it slowly and try not to be deterred if you notice possible mild reactions. Go back down a stage and get some support from a dietitian – Nathalie Newman, Allergy mum and advocate.
How does the milk ladder work day to day?
There are many versions of the milk ladder available. There are different ones for immediate (IgE) and delayed (non-IgE) milk allergy so the day to day may depend on your child’s allergic history. The table shows how you may be asked to introduce milk protein back into the diet if your child has an immediate milk allergy.
Delayed (non-IgE) cows milk allergy has other milk ladders available. Introductions may move faster than the guidance for immediate (IgE) milk allergy but this depends on your child’s symptoms. A slow cautious approach is advised for all types of milk allergy.
The aim for both milk ladders is for foods containing milk that can be tolerated should be part of your child’s diet on a regular basis and not only given occasionally.
Your healthcare professional will advise the reintroduction of cow’s milk for your child when they are ready.
The milk ladder is based on the fact that ‘baked’ cow’s milk protein is usually less allergenic than fresh cow’s milk. The more ‘baked’ the protein, the less allergenic it is. Therefore, the food on the ladder starts with a very well baked milk protein, then the further steps give examples of gradually less baked milk protein products until finally fresh milk is given.
Before starting the ladder, your child must be well with no tummy or skin symptoms and with healthy bowels (their normal poos). Start early in the day and not before bedtime so that you can keep an eye on your child.
Step one is often with a malted milk biscuit (do not use a biscuit with any type of undercooked cow’s milk, for example a cream filling or chocolate). You could also try a savoury option such as those found in the provided iMAP recipes. When starting, your healthcare professional will advise how much of the biscuit to try, as this will depend on your child. It may range from a small crumb to a slightly larger amount. If there have been no symptoms, you’ll be advised to continue to give small amounts of biscuit, gradually increasing the amount. This may take several weeks. After this first step, you’ll then be able to move to the following steps with the guidance of your healthcare professional.
Most children will start on step 1, but if your child is already eating foods on the ladder, you’ll be advised which step you should start on. The ladder has several steps, but your healthcare professional may adjust the number of steps to suit your child. The time spent on each step will depend on how your child responds and this can also be discussed with your healthcare professional.
As your child can tolerate the food at each step, you’ll be able to move to the next step while continuing to feed foods from the previous steps. If your child shows an allergic reaction at any step, you’ll go back to the food on the step before.
Will my child outgrow cow’s milk allergy?
Fortunately, sensitivity to cow’s milk decreases with age1 as most children outgrow their cow’s milk allergy.2 Children with delayed reaction cow’s milk allergy are likely to outgrow their allergy more quickly than those with immediate onset’, while it may take longer for children with immediate onset cow’s milk allergy.3 The speed with which allergies resolve varies from child to child,2 but most children will outgrow their cow’s milk allergy by the time they are five years old.
What can I do to help manage my child’s allergy?
Remember that getting your child back to cow’s milk may help them outgrow their allergy sooner and assists their growth and development.1 You can support this by following the milk ladder for delayed milk allergy in conjunction with healthcare advice, step by step, until your child can tolerate fresh cow’s milk without a reaction. For children with immediate milk allergy this must be guided by a healthcare professional, such as an allergy doctor/ nurse or dietitian and a different process to the milk ladder will be used. For some children, this may be a slow process but keeping any milk protein they can tolerate in the diet every day will help. A broad range of foods in the diet is also important to support overall health.
My child is over five and has an ongoing milk allergy. What is the likelihood they will outgrow the milk allergy?
For some children, especially if they have an immediate milk allergy (IgE), it may have been decided that they continue to exclude milk from their diet for safety reasons or because they have not been able to tolerate baked milk. There is evidence in research to indicate that some children go on to outgrow their milk allergy, even in their teenage years. It is important to continue to have your child reviewed at medical appointments to check tolerance, nutrition and further possible pathways.
What support is there for older children with foods allergies?
If your child is older with a milk allergy then you will want to support your child in dealing with their allergy and encouraging independence. Perhaps they are moving to secondary school and you both need ideas on how to navigate and support this process: Starting a new school with allergy.
A review of your child’s management plan continues to be important for immediate IgE food allergy, an example of a management plan for immediate food allergy would be from BSACI: Paediatric Allergy Action Plans.
On occasions, your older child may be worried and in need of support to deal with their food allergy. This Factsheet, written by a psychologist, offers some suggestions to support your child’s anxiety or top tips for older students.
Starting school, whether primary or secondary, can be a daunting experience for both parents and children. If a ‘new starter’...
How can I support my child’s diet if they are older whilst on a milk free diet?
You may be concerned about whether their diet is properly balanced for an older child and here are a few key pointers. Encourage a wide range of foods to support the gut and overall health:
Protein can be found in many other foods like meat, fish, egg or vegetable proteins (lentils, chickpeas or beans) and often can
be met easily if having a varied diet despite being milk free.
Calcium is needed for health and bones. From one to three years old calcium requirements are 350mg which can be achieved in around 300ml (10oz) of fortified alternative milk or yoghurt. From four to 10 years of age, requirements are around 500mg daily and from 11to 18 years old calcium requirements rise to 800-1000mg. Fortified alternative milks or yoghurt usually provide 120mg per 100ml. Other good sources include fortified breads, cereals, oily fish, broccoli and oranges. It may not be possible to reach the recommended calcium requirements by diet alone. There are a wide range of age-appropriate calcium supplements available from chemists and supermarkets. Do check the ingredients and seek a full diet assessment from a dietitian to support your child.
Vitamin D helps support calcium absorption and it is recommended to take a supplement containing 10mcg per day.
Iodine is important for growth and metabolism. Not all alternative milks are fortified with this so look for ones that are. Other good dietary sources include fish and shellfish.
Are there any new interventions on the horizon for persistent immediate milk allergy?
Research continues to find ways to help children outgrow food allergies. Immunotherapy is one option that we hope will be available to children with persistent immediate (IgE) milk allergy in the future. Immunotherapy is often referred to as ‘desensitisation’ and it is a unique treatment for allergic diseases. It involves giving increasing doses of the allergen at regular intervals (starting with a very small dose) in a carefully controlled way. It may be possible to teach the immune system to tolerate the allergen and not ‘fight’ it.
All immunotherapy carries a degree of risk and it is time-consuming. It can only be undertaken by allergy centres that have extensive experience with immunotherapy. This approach to food desensitisation is mainly in the research stage, but it does provide hope for those at risk of severe food allergic reactions. Learn overall information about immunotherapy here.
How do I get more support?
Remember to stay positive, think healthy and persevere on your journey.
If things feel difficult or overwhelming, reach out to family, healthcare professionals and the helpful links we’ve provided across these Milestones.
We’re also here to help, so please call us for a chat or advice, on the Allergy UK Helpline: Monday to Friday, 9am to 5pm 01322 619 898 or email: [email protected]
The information in this toolkit has been prepared by Allergy UK and peer reviewed by leading experts in cow’s milk allergy. It is designed to be a helpful resource to explain further the types of milestones your child may reach after a diagnosis of cow’s milk allergy. The guidance provided is based on current best practice, but please note that it is subject to change in the light of new relevant information and it does not replace medical/clinical advice. Always speak to your healthcare professional about any concerns you may have about managing the needs of a child with cow’s milk allergy.
With thanks to Nathalie Newman, allergy mum and advocate, for her valuable contribution.
Made possible with support from Mead Johnson Nutrition.