Helpline
Helpline







Types of urticaria and hives
The many different clinical forms of urticaria and they can be divided according to their duration into acute (less than 6 weeks) and chronic (more than 6 weeks) and other.
Acute spontaneous urticaria
- The most common form of urticaria is acute urticaria or “acute spontaneous urticaria”, which lasts a maximum of six weeks (usually a few days to three weeks) and is usually easy to treat. In some patients, angioedema (swelling of deep skin) also occurs. Severe acute spontaneous urticaria may also be accompanied by fever, headache, diarrhea, difficulty in breathing and swallowing, joint pain, and tiredness/fatigue.
Chronic spontaneous urticaria
- If urticarial symptoms—redness, hives, and itching—persist much longer than 6 weeks, it is called chronic spontaneous urticaria. Discomfort can persist for several months or years. Angioedema can also occur, especially in the facial area or on the hands and feet, and in the genital area.
Other types of urticaria include;
- Urticaria factitia can be caused by rubbing, scratching, or scrubbing the skin.
- Cold urticaria occurs when there is contact between the skin and cold.
- Heat urticaria occurs when contact between the skin and warmth/heat.
- Solar urticaria is caused by UV light or sunlight.
- Pressure urticaria presents with swelling at sites of pressure.
- Aquagenic urticaria occurs when there is contact between the skin and water.
- Cholinergic urticaria presents where contact between the skin and raised temperatures (for example hot baths) occurs.
- Exercise-induced urticaria/anaphylaxis occurs during instances of physical strain.
Symptoms of urticaria
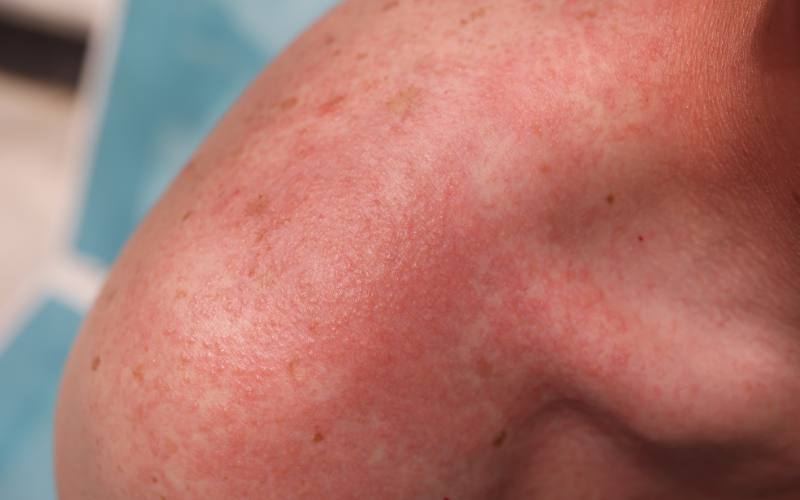
Urticaria can appear suddenly, often without warning. You may wake up one morning to find red, raised welts on your skin, or they may develop rapidly throughout the day. The welts associated with urticaria are usually accompanied by intense itching. This itching can be so severe that it becomes difficult to focus on anything else, and scratching may provide only temporary relief.
The main symptom of hives is an itchy rash and the rash can appear as;
- Raised bumps or patches in many shapes and sizes.
- Appear anywhere on the body.
- Be on one area or spread across the body.
- Feel itchy, sting or burn.
- Look pink or red when affecting someone with white skin; the colour of the rash can be harder to see on brown and black skin.